Arrhythmogenic right ventricular cardiomyopathy (ARVC)
What is ARVC?

- Arrhythmogenic right ventricular cardiomyopathy (ARVC) is a rare heart condition. It is also known as arrhythmogenic right ventricular dysplasia (ARVD), and arrhythmogenic cardiomyopathy (ACM).
- It affects fewer than 200,000 people in the U.S.1
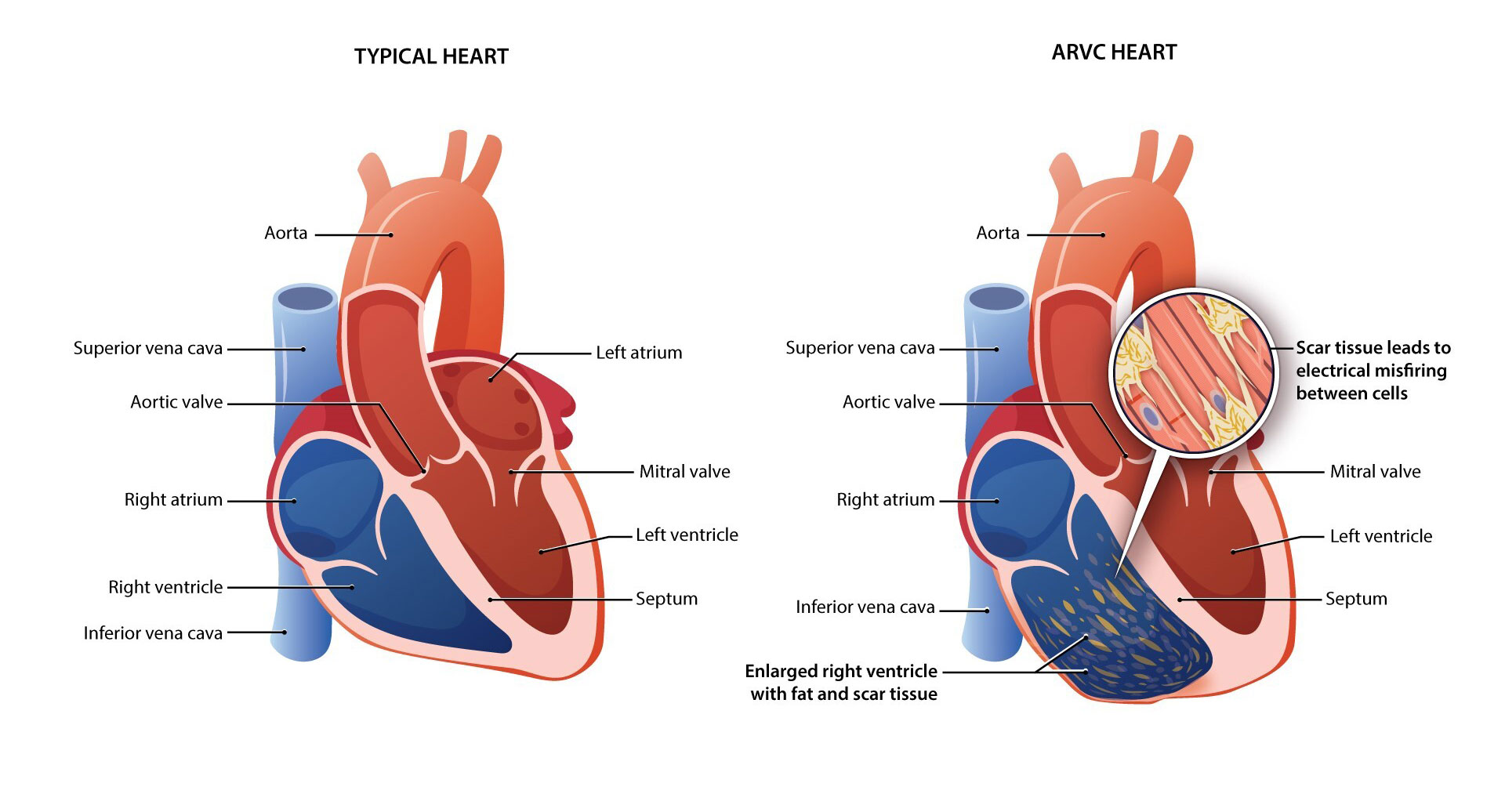
- ARVC occurs when the structure and electrical signals of heart muscle cells, called cardiomyocytes, are disrupted. In a person with ARVC, heart cells lose their structure over time and this can lead to heart failure. The heart cells may also lose their ability to communicate, causing irregular heart rhythms, called arrhythmias. Arrhythmias may feel like a fluttering or racing sensation in the chest, or they may go unnoticed. Episodes are frequently associated with physical exertion.2
- If the rhythm of the heart abruptly stops, this is called sudden cardiac arrest.3,4
- Arrhythmias may go undetected and sudden cardiac death is sometimes the first symptom of disease, particularly in young athletes.1,5
- Symptoms of ARVC include:1,6
- palpitations (feelings that a person’s heart is skipping a beat, fluttering, or beating too hard or too quickly)
- lightheadedness
- dizziness
- fainting after physical activity
- shortness of breath.
- ARVC symptoms are most commonly recognized between the ages of 10 and 50 years, with an average age at diagnosis of about 30 years.7-10
- The median age of cardiac arrest in people with ARVC is 25 years old.7
- ARVC is a progressive disease, meaning that once someone becomes symptomatic, their symptoms usually do not go away, and over time their condition is likely to get worse, possibly affecting other functions of the heart.10

What causes ARVC?
Almost half of ARVC cases are caused by genetic mutations in certain heart muscle genes.11 Mutations in a gene can affect that gene’s ability to make a protein the way it should. It can also affect whether that protein is made at all. When not enough protein is made, or no protein is made, the heart muscle cells don’t work properly.
Mutations in Genes Cause ARVC

The most common cause of ARVC is a mutation in a gene called plakophilin-2, or PKP2.11
- The PKP2 mutation is found in about 45% of people diagnosed with genetic ARVC in the U.S.11
- Changes in the PKP2 gene can prevent the heart muscle cells from making enough of the PKP2 protein, which works with other proteins to support the structure and communication of heart muscle cells.12
A Closer Look at How ARVC Affects the Heart
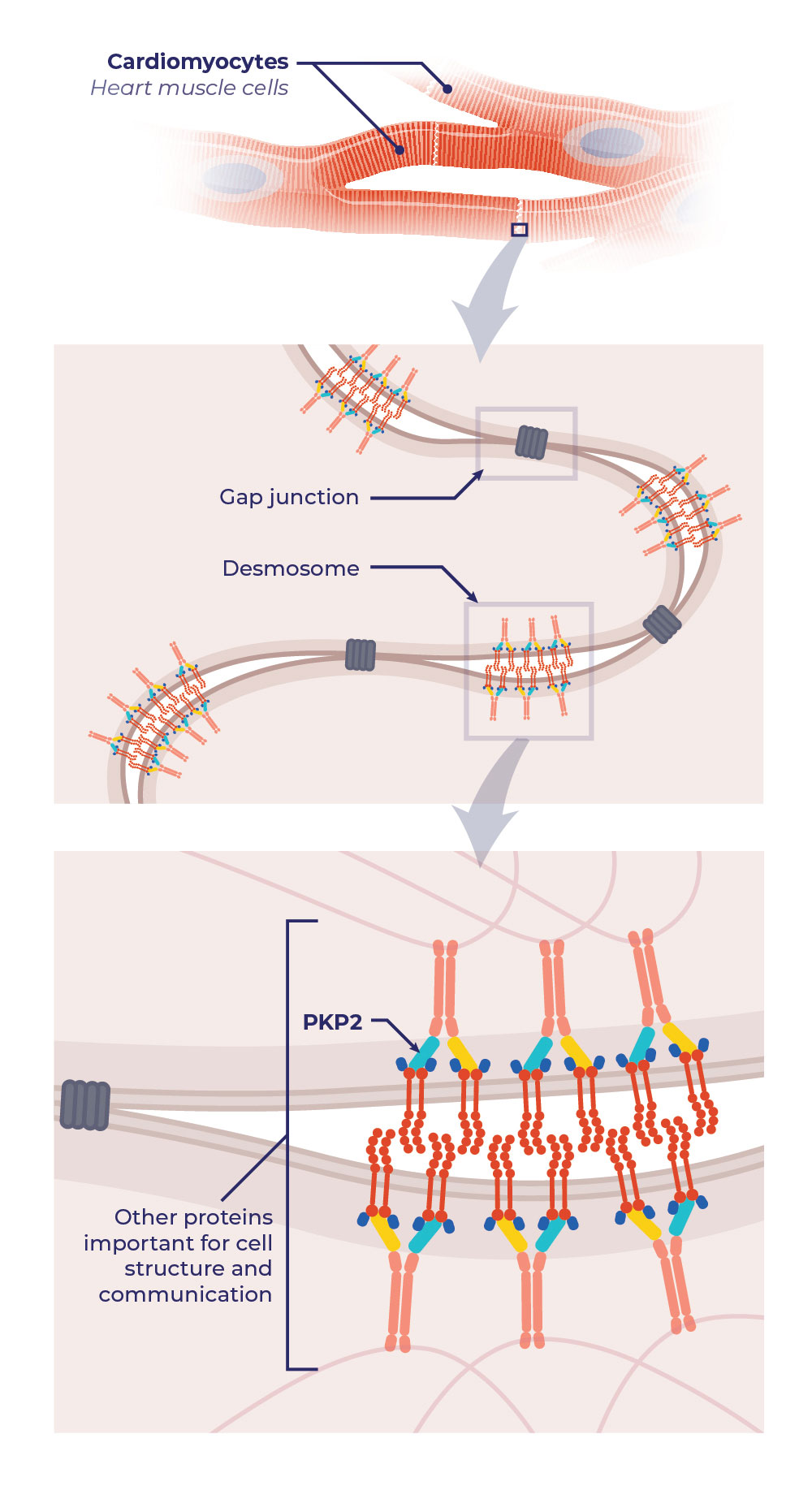
Mutations in the PKP2 gene can prevent the heart muscle cells from making enough of the PKP2 protein, which works with other proteins to support the structure and communication of heart muscle cells.12
Desmosomes and gap junctions of heart muscle cells are important for cell structure and communication.
Desmosomes provide structural support by connecting heart muscle cells together.
Gap junctions communicate electrical signals between heart muscle cells.13
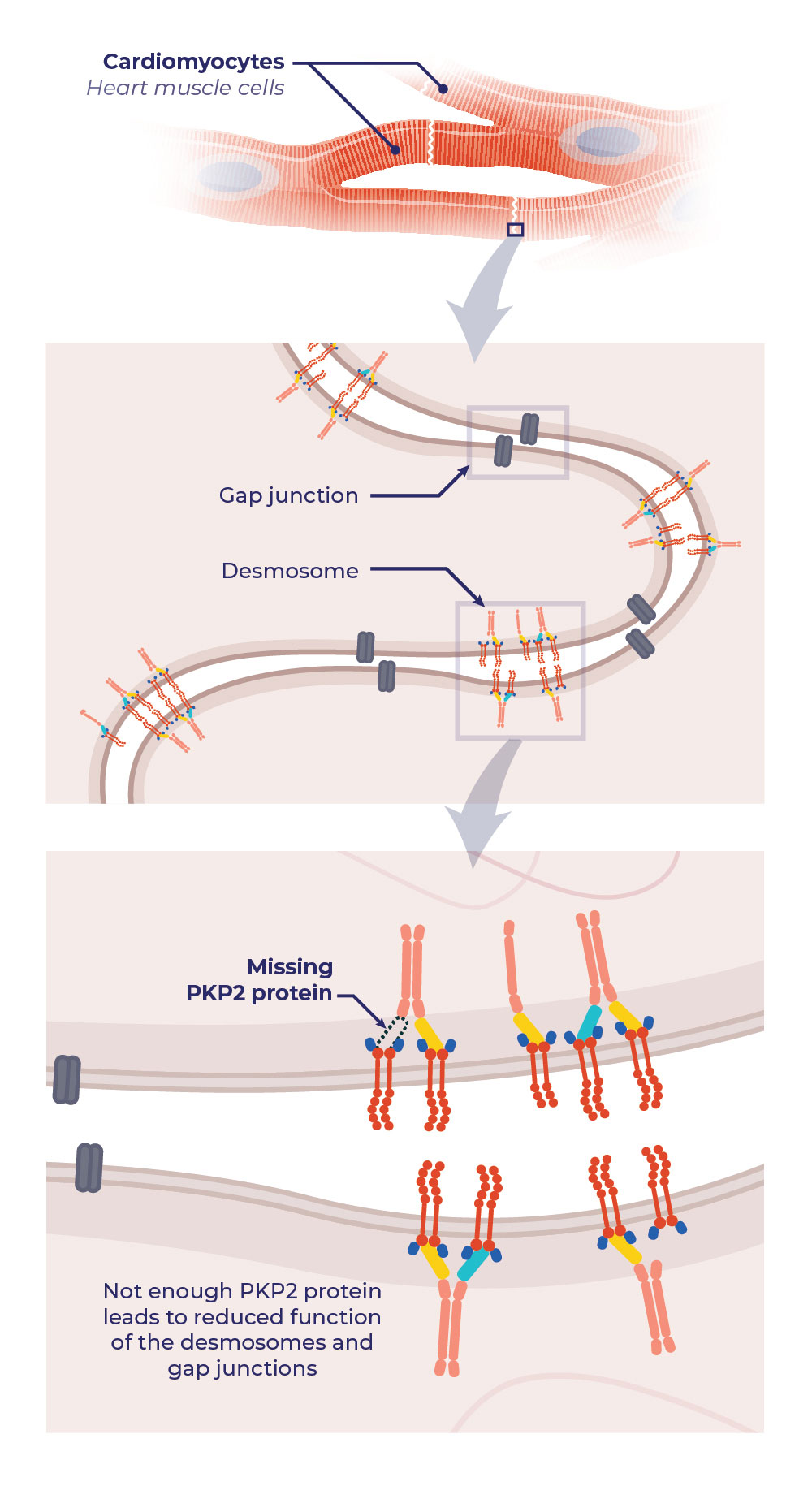
When a person has a PKP2 mutation and does not make enough PKP2 protein, gap junctions and desmosomes are affected.
- When the heart muscle cells lose their structural connections, the heart muscle becomes weaker and may develop a type of scar tissue that is unique to ARVC. This can lead to heart failure.
- When the heart muscle cells lose their electrical communications, the electrical pulses can become unstable and cause irregular heart rhythms (called arrhythmias). This can lead to sudden cardiac death.13
Typical Heart Cells
ARVC Heart Cells
Inheritance Pattern of ARVC14
Genetic mutations for ARVC are usually passed down, or inherited, from one parent who carries the genetic mutation.5,11
- A child can develop ARVC if they receive a single copy of the PKP2 mutation from one parent. This is called an autosomal dominant inheritance pattern.
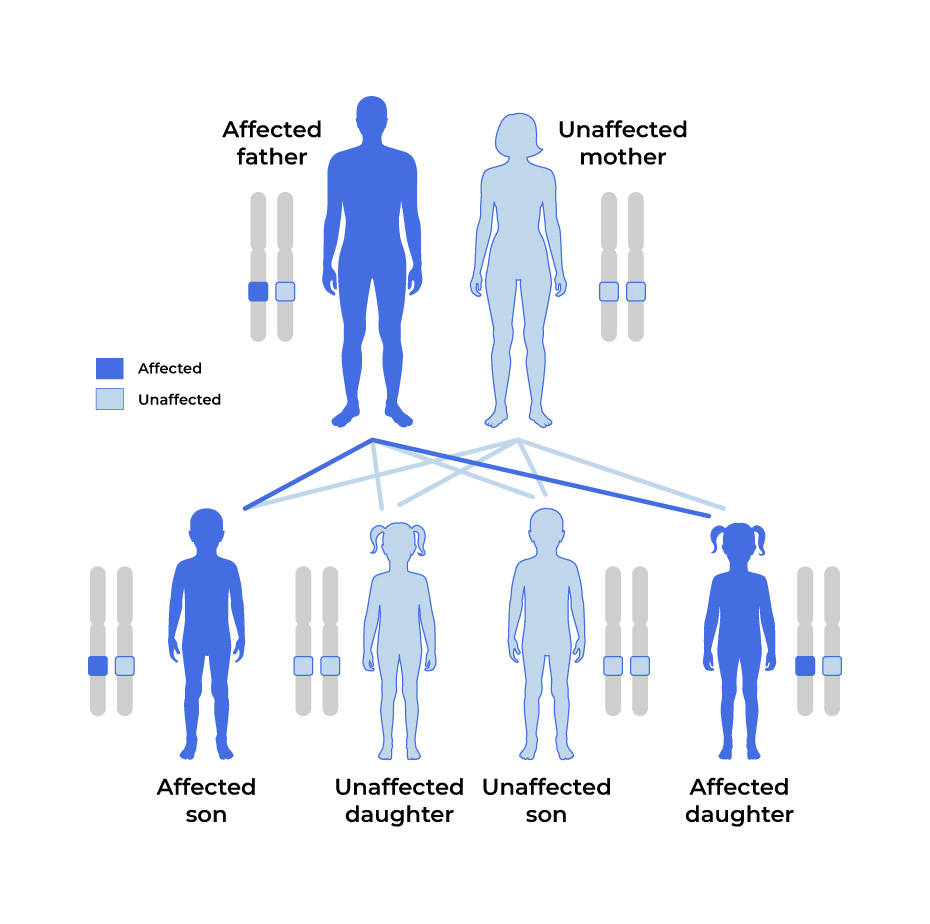
Autosomal Dominant
In most cases of ARVC, the genetic mutation is carried by one parent and passed down to children.
With an autosomal dominant pattern, there is a 50% chance of passing the mutation down to a child.
People who have been diagnosed with ARVC but who don’t yet know their specific mutation should talk to their cardiologist, primary care physician, or a genetic counselor about genetic testing. Click here for more information about genetic testing.
What are the symptoms of ARVC?

The most common symptoms of ARVC include:1
- Arrhythmias (irregular heart rhythms), including
- Premature ventricular contractions, a type of irregular, extra heartbeats that begin in one of the heart's two lower pumping chambers (ventricles)15
- Ventricular tachycardia, a type of fast heart rate that starts in the heart’s lower chambers (ventricles). Electrical signals in the heart’s lower chambers fire unusually fast.16
- Non-sustained ventricular tachycardia is another type of heart rate rhythm that is increased over the course of less than 30 seconds
- Lightheadedness
- Palpitations
- Dizziness
- Fainting
- Shortness of breath
How is ARVC diagnosed?
ARVC can be hard to diagnose because there isn’t one test that can confirm the diagnosis. A cardiologist usually needs many different types of information to make a diagnosis of ARVC, including: 10,17
- Family history
- Tests to analyze heart rhythm, such as an electrocardiogram (ECG) or electrophysiology studies
- Tests to analyze the blood flow in the heart and heart motion, such as an echocardiogram (echo)
- Tests to examine the heart anatomy, such as a cardiac MRI
- A biopsy to collect heart muscle cells so they can be looked at in a lab for more details
- Results from genetic testing
- Results of genetic testing may reveal that a person has genetic mutations known to cause ARVC, even if they have not experienced ARVC symptoms.
- If a person knows that one of their relatives has ARVC, they should tell their doctor.
- In either case, it may be helpful to consult with a specialized cardiologist or a comprehensive ARVC center. Specialists or comprehensive care centers can:
- Recommend a plan to monitor a person’s heart,
- Make suggestions on how to best take care of themselves,
- Have knowledge of or access to the latest treatments and clinical trials, and
- Help a person find a genetic counselor.
What is the role of a genetic counselor?
A genetic counselor is a healthcare professional that a person may see as part of the genetic testing process. Genetic counselors can help explain:
- The genetic testing process and possible outcomes
- How a condition is inherited
- Individual test results
- The chance of passing a gene mutation on to a child
How can I find a genetic counselor?
Consult with your physician or find more information here.
Expand for References
1. Arrhythmogenic right ventricular cardiomyopathy. U.S. Department of Health and Human Services, National Institutes of Health, National Center for Advancing Translational Sciences, Genetic and Rare Diseases Information Center; 2024. https://rarediseases.info.nih.gov/diseases/5847/arrhythmogenic-right-ventricular-cardiomyopathy. Accessed April 15, 2024. 2. Arrhythmia. American Heart Association; 2022. https://www.heart.org/en/health-topics/arrhythmia. Accessed June 17, 2024. 3. Cardiac Arrest Causes and Risk Factors. U.S. Department of Health and Human Services, National Institutes of Health National Heart, Lung, and Blood Institute; 2022. https://www.nhlbi.nih.gov/health/cardiac-arrest/causes. Accessed April 15, 2024. 4. Cardiac arrest. American Heart Association; 2023. https://www.heart.org/en/health-topics/cardiac-arrest. Accessed April 15, 2024. 5. Shah SN, Umapathi KK, Oliver TI. Arrhythmogenic right ventricular cardiomyopathy. In: StatPearls [Internet]. StatPearls Publishing; 2023. https://www.ncbi.nlm.nih.gov/books/NBK470378/. 6. Arrhythmogenic right ventricular dysplasia. American Heart Association; 2022. https://www.heart.org/en/health-topics/cardiomyopathy/what-is-cardiomyopathy-in-adults/arrhythmogenic-right-ventricular-dysplasia. Accessed April 15, 2024. 7. Groeneweg JA, Bhonsale A, James CA, et al. Clinical presentation, long-term follow-up, and outcomes of 1001 arrhythmogenic right ventricular dysplasia/cardiomyopathy patients and family members. Circ Cardiovasc Genet. 2015;8:437. https://doi.org/10.1161/CIRCGENETICS.114.001003 8. Dalal D, Nasir K, Bomma C, et al. Arrhythmogenic right ventricular dysplasia: a United States experience. Circulation. 2015 ;112:3823. https://doi.org/10.1161/CIRCULATIONAHA.105.542266 9. Nava A, Bauce B, Basso C, et al. Clinical profile and long-term follow-up of 37 families with arrhythmogenic right ventricular cardiomyopathy. J Am Coll Cardiol. 2000;36:2226-2233. https://doi.org/10.1016/s0735-1097(00)00997-9 10. Hulot JS, Jouven X, Empana JP, et al. Natural history and risk stratification of arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circulation. 2004;110:187. https://doi.org/10.1161/01.CIR.0000143375.93288.82 11. Jacob KA, Noorman M, Cox MG, et al. Geographical distribution of plakophilin-2 mutation prevalence in patients with arrhythmogenic cardiomyopathy. Neth Heart J. 2012;20(5):234-239. https://doi.org/10.1007/s12471-012-0274-x 12. van Tintelen JP, Entius MM, Bhuiyan ZA, et al. Plakophilin-2 mutations are the major determinant of familial arrhythmogenic right ventricular dysplasia/cardiomyopathy. Circulation. 2006;113:1650-1658. https://doi.org/10.1161/CIRCULATIONAHA.105.609719 13. Austin KM, Trembley MA, Chandler SF, et al. Molecular mechanisms of arrhythmogenic cardiomyopathy. Nat Rev Cardiol. 2019;16(9):519-537. https://doi.org/10.1038/s41569-019-0200-7 14. Overview of inheritance. American Heart Association. https://www.heart.org/-/media/Files/Health-Topics/Cardiomyopathy/Cardiomyopathy-Inheritance-UCM_312228.pdf. Accessed April 15, 2024. 15. Premature Contractions – PACs and PVCs. American Heart Association; 2022. https://www.heart.org/en/health-topics/arrhythmia/about-arrhythmia/premature-contractions-pacs-and-pvcs. Accessed April 15, 2024. 16. Tachycardia: Fast Heart Rate. American Heart Association; 2022. https://www.heart.org/en/health-topics/arrhythmia/about-arrhythmia/tachycardia–fast-heart-rate. Accessed April 15, 2024. 17. Arrhythmogenic right ventricular cardiomyopathy. Cedars Sinai. https://www.cedars-sinai.org/health-library/diseases-and-conditions/a/arrhythmogenic-right-ventricular-dysplasia.html. Accessed April 15, 2024. 18. Towbin JA, McKenna WJ, Abrams DJ, et al. 2019 HRS expert consensus statement on evaluation, risk stratification, and management of arrhythmogenic cardiomyopathy. Heart Rhythm. 2019;16;e301-e372. https://doi.org/10.1016/j.hrthm.2019.05.007 19. Arbelo E, Protonotarios A, Gimeno JR, et al. 2023 ESC Guidelines for the management of cardiomyopathies: Developed by the task force on the management of cardiomyopathies of the European Society of Cardiology (ESC), European Heart Journal, 2023; https://doi.org/10.1093/eurheartj/ehad194